Clinics assumed radiologists would reject an unfamiliar platform. Radiologists assumed clinics would send incomplete scans. Both groups were designing around the risk of the other person failing. Speed was never the problem.

01 — Business Context
Why This Problem Mattered Now
Radiology workflows relied on physical CD or printed results delivery — creating delays, limiting specialist access, and introducing operational risk. The opportunity: build the country's first digital radiology network.
The Risk
Medical data is highly regulated. A poorly designed platform could break trust or create failures harder to detect than manual processes.
If Left Unsolved
Clinics would continue relying on slow physical delivery. Diagnostic turnaround would remain measured in days, and specialist access would depend on geography.
Stakeholders
Clinic administrators, radiologists, heads of radiology departments, medical directors, compliance and legal teams, product and engineering.
The Central Tension
The business wanted to replace a slow, expensive process with a digital workflow. Users needed certainty that the new system would not create new risks. Speed alone was not enough — trust and reliability were essential.
Success metrics: adoption, diagnostic turnaround time, specialist network growth, workflow efficiency, and transition away from physical delivery.
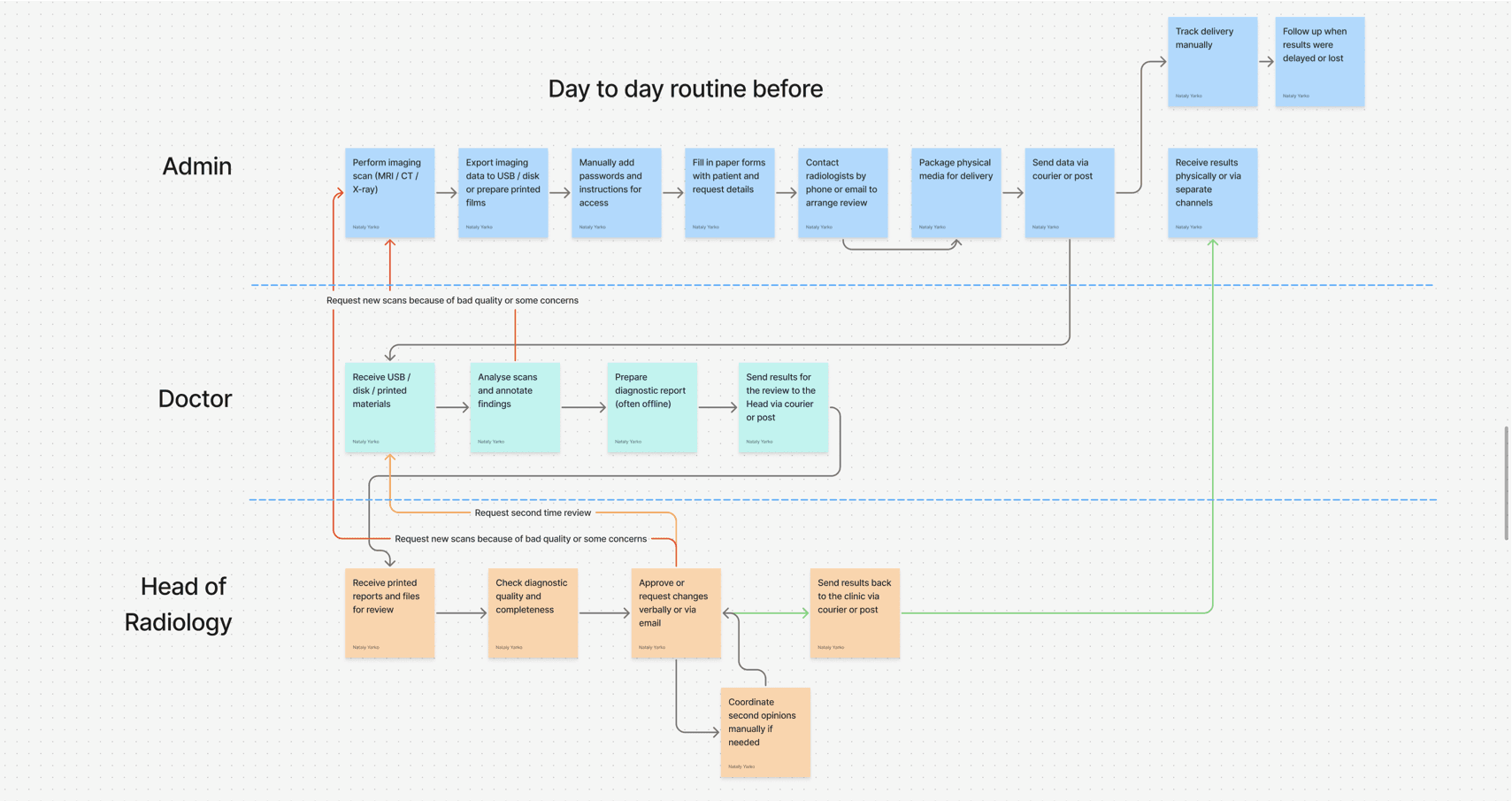
The physical delivery process
12 days from scan to final result, with multiple delivery trips and waiting states. No tracking, no recovery if documents got lost.

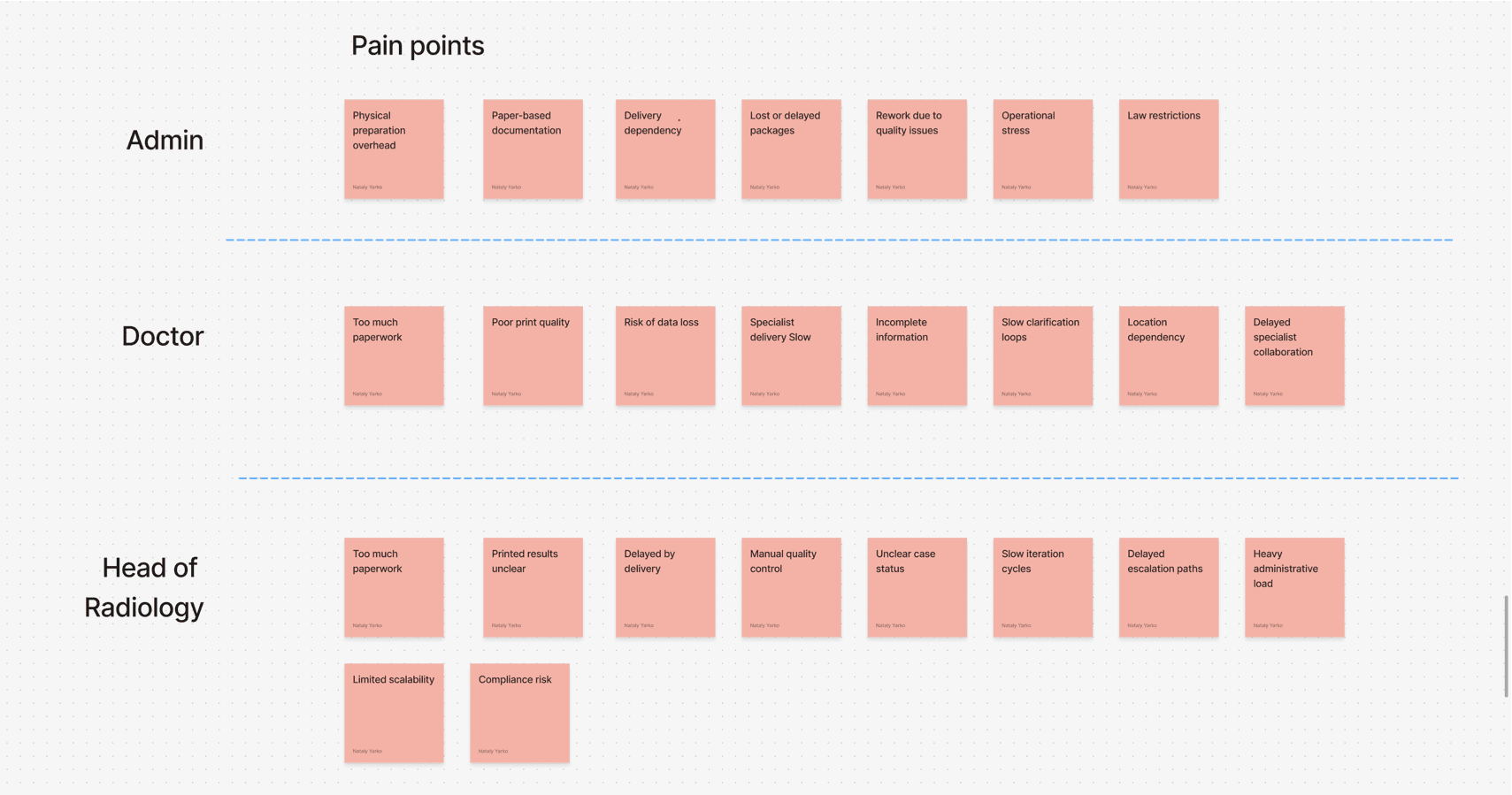
02 — Problem
What We Believed vs. What We Discovered
The Business Problem
Physical delivery of scans prevented efficient scaling. Turnaround times were slow, coordination was manual, and expanding specialist access was difficult.
The User Problem
Clinics lacked case visibility. Radiologists had limited coordination. Documents could be lost. Nobody had a reliable view of where a case was in the diagnostic process.
Initial Assumption
We believed the core challenge was replacing physical transfer with digital transfer. If we could securely upload and distribute imaging files, the main problem would be solved.
What Research Revealed
Users understood the existing process's limitations and knew how to work around them. What concerned them was that a digital system would fail in ways they could not see, understand, or recover from.
What Turned Out To Be Wrong
We assumed that secure digital file transfer would solve the problem. It wouldn't. The real problem was that users couldn't trust a system that failed silently.
The Pivot
The challenge was no longer moving files faster. It was designing a workflow that users could trust.

03 — My Role
What I Actually Owned
I owned the end-to-end product design process — from discovery research through to the shipped product.
Discovery & Research
Conducted research across all three primary user groups. Tested rough concepts early to uncover workflow conflicts before development began.
Workflow Architecture
Helped move the team from a file-based model to a case-based workflow model — supporting ownership, visibility, and recovery. Defined how diagnostic work would move safely and predictably.
Design System
Created a design system supporting three distinct user groups: clinic administrators, radiologists, and heads of radiology departments.
Collaboration & Constraints
Worked with 1 BA, 1 PM, 4 developers, 1 QA, and legal/compliance stakeholders.
Healthcare regulations influenced almost every product decision.
How I shaped direction
After research, I proposed two decisions the team hadn't planned for. First, a case-based architecture instead of file transfer — I brought this to the engineering lead, we prototyped it together before anyone touched the design system. Second, a scoped mobile app for radiologists: not a full product, just case summaries and one-tap accept/decline. The full review stayed on desktop. Both decisions came from the same research insight — radiologists needed to stay in control without being overwhelmed.


Timeline
2021
MVP delivered within a 6-month timeline.
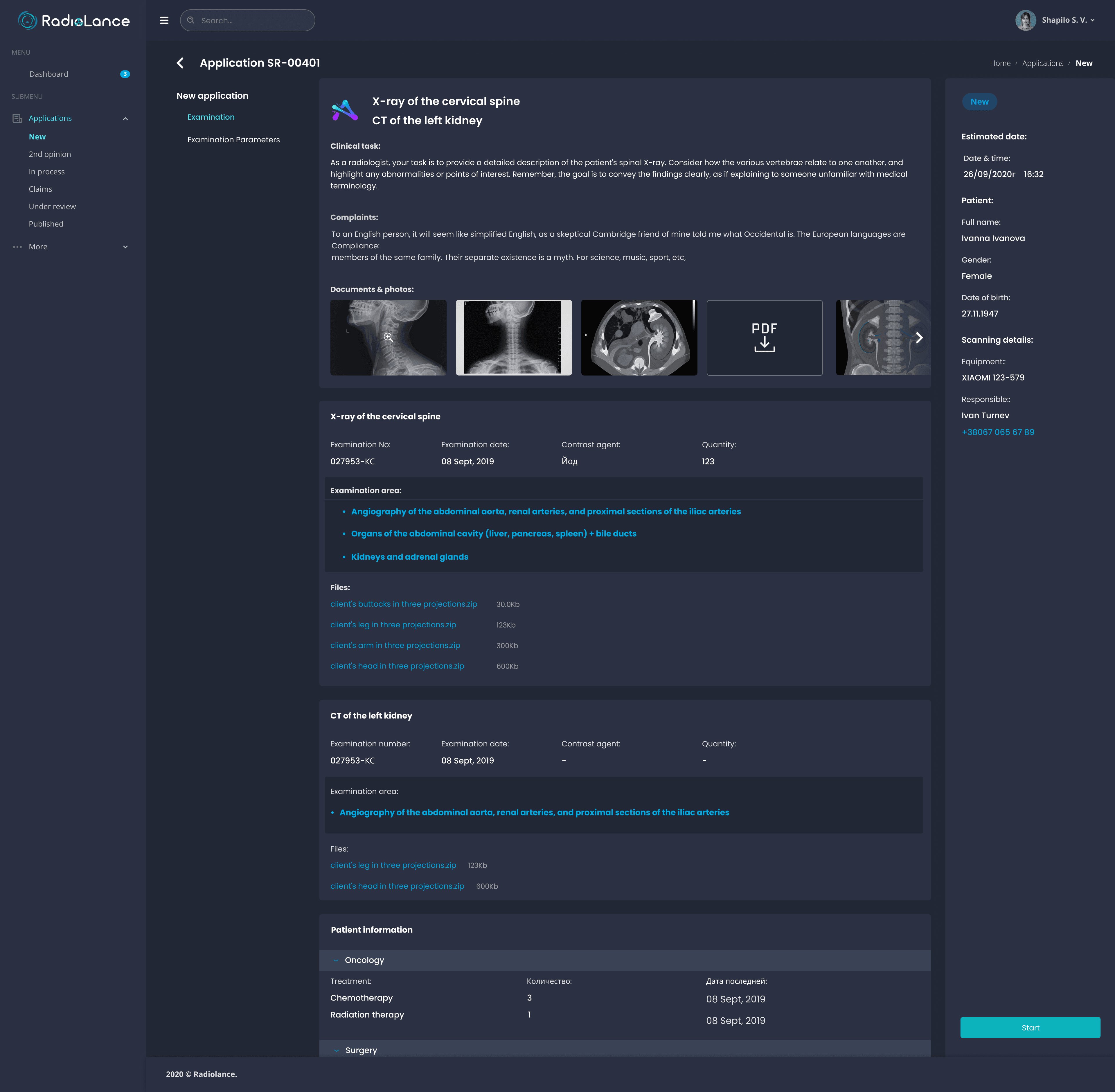
04 — Direction
The Decision
We decided to build a case-based radiology platform rather than a file-sharing system.
Instead of simply transferring medical images between clinics and radiologists, the platform would manage the entire diagnostic workflow. Every case would have ownership, status, history, notifications, and clearly defined handoffs between participants. The goal was to create a system where work could be tracked, monitored, reassigned, and recovered when problems occurred — making the workflow trustworthy as well as efficient.
Case workflow architecture
Cases move through the system with clear handoffs between roles. Notifications trigger at each step (10m-15m, 5m-15m timing shown in blue), decision points handle edge cases (need second opinion?), and every state is visible and recoverable. This architecture made failures visible instead of silent.

Files model
A file moves. Nobody owns it.
No status. No history.
If a radiologist goes offline — case disappears.
Failure is silent.
Cases model
A case moves. Someone always owns it.
Status, history, handoffs at every step.
If a radiologist goes offline — case is reassigned.
Failure is visible and recoverable.


05 — Impact
Why This Project Matters
1,500+
Diagnostic cases
Processed within six months of launch
70+
Radiologists
Joined the specialist network
15+
Clinics across major cities
Adopted the platform
150+
Reports per day
Platform remains in use today across public and private clinics
The platform remains in use today — the strongest indicator of lasting impact. It also influenced how stakeholders thought about digital transformation: rather than digitising existing paperwork, the team redefined how diagnostic work itself moved through the organisation.
"As the medical director of a private clinic, I appreciate the speed and predictability of working with Rad!oLance. Every day, we receive mammography and X-ray descriptions at the agreed time. If necessary, we request urgent descriptions within 2 hours. It is also very important for us that Rad!oLance operates officially based on a contract. A reliable and time-tested partner."
T. Bulanov,
Director of “Medibor” Clinic
"We have been working with Rad!oLance for over two years. They always take a thorough approach to describing and interpreting CT/mammography results. Deadlines have never been missed. During our collaboration, the number of orders has increased by 30%, which indicates trust from both doctors and patients."
A. Kovalyov,
Head of Valky Central District Hospital
This is the condensed version.
Want the full srory?
The deeper sections cover: why a file-based model fundamentally couldn't work and what replaced it, a design principle I'd push back on next time (launching across all clinics at once instead of a single pilot), and the core lesson — that in high-stakes workflows, trust is built through failure handling, not the happy path.
Happy to walk you through the complete story at interview.


