Feature design
B2B2C Healthcare
COVID-19 Response
Telemedicine
The core challenge was trust across three user types with completely different needs: patients booking remotely, clinic admins coordinating schedules, and doctors managing cases across two systems simultaneously.

01 — Business Context
Why This Problem Mattered Now
The Gap
Two established healthcare platforms — Medstar (doctor MIS/EHR) and Medcard24 (patient portal, owned by SK-Telemed) — operated with no connection between them. Neither supported remote workflows. Patients could not consult doctors remotely, request prescriptions online, or communicate outside physical appointments. When COVID-19 lockdowns began, this became critical. Doctors were seeing 48-50 patients per 8-hour shift — around 10 minutes per patient — and regularly staying longer when complex cases demanded more time. High-risk and elderly patients could not access care safely in person, but there was no remote alternative.
Risk & Opportunity
Clinics were overloaded, doctors faced burnout, and patients delayed treatment due to safety concerns. The opportunity was to establish a telehealth ecosystem extending care beyond physical clinics.
Stakeholders
Doctors · Patients · Clinic Administrators · Product Manager · Business Analyst · Development Team
Success Metrics
Enable remote healthcare delivery at scale — measured through adoption of remote consultations, reduction of offline visits, improved accessibility, and supporting doctors under lockdown conditions.
The business needed telemedicine delivered quickly to keep services operational during lockdowns. Users needed accessibility regardless of age, technical literacy, or device limitations. Early assumptions favoured video consultations, but research revealed many patients lacked webcams and elderly users struggled with video technology.
Lockdowns made in-person care dangerous and unsustainable. Doctors were seeing over 150 patients a day with no remote alternative. Patients stayed home and went without care. The system needed a digital escape route, fast.
Doctor Burnout Risk
Unsustainable patient volume with no way to reduce in-person load
No Remote Option
The platform had no consultation flow outside physical visits
Elderly Patients Stranded
High-risk patients couldn't safely access care
Zero Scheduling Infrastructure
No digital way to manage or redistribute appointment load
02 — Problem Space
The Problem We Were Solving
The Business Problem
Medstar and Medcard24 operated as separate systems with no integrated telehealth infrastructure. Neither platform supported remote consultations, online appointment booking, prescription requests, or doctor-patient communication outside clinic visits.
The User Problem
Patients could not access healthcare remotely, request prescriptions online, communicate with doctors between appointments, or monitor their health over time. Doctors had no way to reduce in-person workload, conduct remote consultations, or manage increasing patient demand efficiently.
What We Assumed
We assumed video consultations would become the primary method and that connecting the two products would solve most lockdown challenges.
What We Didn't Know
We lacked data about patient technology access, consultation preferences, adoption barriers, the needs of elderly users, and how doctors would adapt to telemedicine workflows under crisis conditions.
What Proved Wrong
A large proportion of patients did not have webcams — a video-first experience would exclude many users who needed remote healthcare most.
"I couldn't get an appointment without calling during work hours. By the time I got through, all slots were gone."
— Maria K. · Patient, 34
— Dr. Olena V. · Family Doctor,
Kyiv clinic
"Scheduling was completely manual. Doctors were overwhelmed and I had no visibility into who was coming or when."
— Andriy S. · Clinic Administrator
A video-first experience would have excluded the patients who needed remote care most. Chat had to become a first-class channel, not a fallback.
03 — My Role
What I Actually Owned
Scope
I worked as an outsourced designer through SDH, embedded across both Medstar and Medcard24. I owned the end-to-end design process: user research, information architecture, user flows, UX design, UI design, prototyping, usability testing, and developer handoff.
Collaboration
1 Product Manager · 1 Business Analyst · 4 Developers · 1 QA Engineer
Products
Medstar (doctor MIS/EHR) · Medcard24 (patient portal) · IDIS2GO (telehealth diagnostic system) · Show2Doc (doctor-to-patient communication platform)
Influence
Beyond execution, I helped shape product direction through research findings. I advocated for making chat a primary consultation method rather than a fallback to video, and introduced an administrator workflow after identifying operational bottlenecks not addressed in the original scope.
The idea for Show2Doc emerged during the project — a dedicated doctor-to-patient communication platform that went from concept to launch in July 2020.
Timeline
Lockdown in 2020
Phase 1: March-April 2020, 6 weeks — Medstar + Medcard24 connected for telehealth
Phase 2: IDIS2GO integration — telehealth diagnostic system added
July 2020: Show2Doc launched — new product, born from research during the project
04 — Direction
What We Decided to Build
We connected Medstar and Medcard24 into a single telehealth ecosystem — allowing patients to book appointments, consult doctors remotely, request prescriptions, and manage healthcare from home, while enabling doctors and clinics to coordinate care through a connected workflow.





05 — Impact
Why This Project Matters
37K+
Physicians on platform
120K
Appointments/Day at peak
4.8
App Store rating
48%
reduction in offline visits
The platform evolved from disconnected healthcare tools into an integrated ecosystem, creating the foundation for future services including wellness tracking and medication delivery. Medstar covers approximately 15% of the Ukrainian EHR market.
Before
Consultations
In-person visits only · Exposure risk for everyone during lockdown
Appointment Booking
Call the clinic during working hours · Long queues, no visibility
Patient records
Paper files · No digtal access for patients or remote doctors
Doctor workload
150+ patients daily · No way to redistribute or reduce load
VS
After
Consultations
Video callor chat from home via Medcard24 app · No exposure
Appointment Booking
Book online anytime. Admin manages schedule via Medstar dashboard.
Patient records
Full EHR in-app. History, prescriptions, and treatment plans in one place.
Doctor workload
Doctor workload: Distributed across remote and in-person. Offline visits reduced by 48-51%.
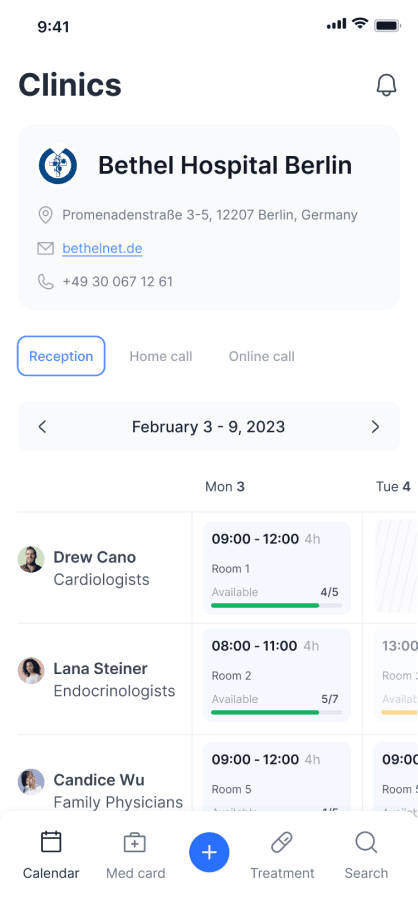
Clinics — Bethel Hospital Berlin, available booking slots. Patient-side booking infrastructure.

This is the condensed version.
Want the full story?
The deeper sections cover: why video-first was rejected after research (it would have excluded the patients who needed remote care most), how an administrator persona emerged mid-project and changed the entire scope, and what I'd validate earlier next time — patient hardware, accessibility for elderly users, and admin workflows, all of which we discovered too late.
Happy to walk you through the complete story at interview.


